
A CIO usually reaches for healthcare IT recruiting firms when a project is already slipping. The Epic optimization workstream needs an analyst who understands clinical workflows. The identity program needs a security engineer who can work inside HIPAA-bound environments. The data platform needs someone who has touched interoperability, not just generic ETL. Internal recruiting posts the role, applicants trickle in, and the hiring team realizes the actual problem isn't volume. It's fit.
That's why this market behaves differently from general tech hiring. In healthcare IT, the candidate has to match the stack, the operating model, and the regulated context. A recruiter who can fill a SaaS sales engineer role won't automatically know how to qualify an interface analyst, an EHR trainer, or a cloud architect supporting protected health information.
Table of Contents
- Why Healthcare IT Hiring Is a Unique Challenge
- First, Define Your True Cost of Vacancy
- How to Vet and Shortlist a Recruiting Partner
- Selecting Your Recruitment Engagement Model
- Defining KPIs and SLAs for Your Recruiting Firm
- Spotting Red Flags and Structuring the Agreement
- From Vendor to Partner Your Long-Term Strategy
Why Healthcare IT Hiring Is a Unique Challenge
A healthcare IT opening rarely fails because the title is unclear. It fails because the underlying requirement sits below the title. A hospital might say it needs a cybersecurity engineer, but its need is for someone who can secure clinical systems, handle privileged access in a regulated setting, and communicate risk to operations leaders who care about uptime as much as policy.
That mix is why healthcare IT recruiting firms exist as a distinct category. The broader staffing market keeps expanding. IBISWorld reports that the number of U.S. Healthcare Staff Recruitment Agencies reached 3,268 in 2024 and is projected to rise to 3,349 in 2025. More firms entering the market usually signals sustained demand, not simplicity.
The role requires two kinds of fluency
Healthcare IT candidates need technical credibility and domain credibility. A strong engineer who has never worked around patient data governance, EHR dependencies, or clinical escalation paths may still struggle. The reverse is also true. Deep healthcare exposure without current technical depth won't move a cloud migration, IAM redesign, or analytics modernization effort forward.
That's why hiring teams often miss when they use generic screening. Resume filters overvalue familiar tools and undervalue context. In healthcare, context often decides whether the person can perform on day one.
Practical rule: If the role touches patient data, regulated workflows, or a clinical platform, treat domain knowledge as part of the core qualification, not as a nice-to-have.
The project risk is operational, not just hiring related
When healthcare organizations miss on a hire, the damage doesn't stop at an empty seat. It shows up in delayed go-lives, overextended analysts, postponed security work, and growing dependence on contractors who were never meant to own the long-term roadmap.
Leaders hiring for security-related functions often start with a narrower search partner because the talent pool is small and the screening burden is high. Teams evaluating those paths often compare recruiter support with the broader market for healthcare cybersecurity jobs to understand where domain-specific talent resides.
Healthcare IT recruiting firms are useful when the organization needs more than candidate flow. They're useful when the organization needs translation between technology, operations, and compliance.
First, Define Your True Cost of Vacancy
Most hiring decisions get framed the wrong way. Finance asks what the agency fee will be. The better question is what the open role is already costing every week it stays vacant.
In healthcare, vacancy cost is rarely just lost output from one person. It spreads. Analysts cover two systems instead of one. Security work gets pushed behind audit remediation. Leaders spend time interviewing weak fits because the funnel isn't producing enough qualified candidates. The team pays in delay, distraction, and burnout.
The market data supports that pressure. CareerPlug's 2022 healthcare recruiting study found 14 applicants per job and an average time to hire of 19.5 days, and SmartRecruiters reported in 2025 that healthcare receives 45% fewer applications per role than the global average. That combination matters. Low volume means the pipeline is thin. Fast cycles mean the good candidates don't wait.
What belongs in the vacancy calculation
A CIO doesn't need a complex finance model to make a sound decision. A practical internal estimate usually includes:
- Project delay cost: Revenue cycle upgrades, EHR optimization, integration work, and security initiatives often stall when one key specialist is missing.
- Team strain: Existing staff absorb extra tickets, escalations, and after-hours work. That increases risk of turnover and lowers quality.
- Compliance exposure: Open roles tied to access controls, audit response, privacy operations, or infrastructure resilience create outsized risk even when the role itself isn't revenue producing.
- Leadership drag: Directors, architects, and managers spend hours re-explaining the role, re-screening resumes, and reopening searches.
A simple decision test
The most useful decision framework is blunt. Use a specialist firm when the weekly cost of vacancy is higher than the likely cost of external search spread across the time the role would otherwise remain open.
That's especially true for positions where a narrow profile matters, such as:
- EHR and EMR roles where certification, build experience, or hospital workflow knowledge can't be learned during onboarding.
- Cybersecurity roles where the person must manage both technical controls and healthcare-specific risk.
- Data and interoperability roles where HL7, FHIR, integration engines, or governed analytics environments shape the work.
- Leadership hires where one bad fit can slow an entire transformation program.
The mistake isn't paying for specialist help too early. It's waiting until the vacancy has already disrupted delivery.
What doesn't work
Several patterns routinely fail in this market:
- Posting broad job descriptions: “Healthcare IT experience preferred” usually invites the wrong audience.
- Treating all applicants as equal: A short list of relevant candidates beats a large stack of generic resumes.
- Moving at standard enterprise speed: If interview scheduling drags, the best candidates accept elsewhere.
For a CIO, the right starting point isn't vendor outreach. It's internal clarity on what delay is costing now.
How to Vet and Shortlist a Recruiting Partner
A healthcare IT recruiter should be able to discuss the role without hiding behind buzzwords. If the firm can't distinguish Epic reporting from interoperability engineering, or cloud modernization from regulated hosting operations, the search will drift immediately.

The vetting process should focus less on brand recognition and more on proof of working knowledge. In this segment, domain fluency matters because the demand profile is changing. Industry guidance notes that the strongest healthcare IT recruiting firms now need evidence of fluency in AI-enabled clinical workflows, cyber risk, cloud migration, and data interoperability within regulated hospital environments.
Questions that reveal real expertise
Use live role discussion instead of generic capability decks. Ask questions that force the firm to show how it thinks.
- Ask for role decomposition: “How would this firm separate must-have healthcare knowledge from trainable technical skills for this search?”
- Test their screening method: “How does the recruiter verify that a candidate has worked in regulated environments, not just listed healthcare on a resume?”
- Probe sourcing depth: “Where does the firm look when the right candidate isn't applying on job boards?”
- Check forward-looking skill awareness: “How would the firm screen differently for legacy EHR support versus a cyber or interoperability role?”
A capable partner answers with specifics. It should mention workflow exposure, stakeholder environment, screening sequence, and likely candidate trade-offs. It shouldn't default to “large network” and “proprietary database.”
What to ask for during the shortlist stage
A serious evaluation usually includes evidence in four areas:
| Evaluation area | What good looks like | What to avoid |
|---|---|---|
| Role understanding | The recruiter can restate the role in operational terms | They repeat the job description back verbatim |
| Candidate qualification | Clear screening for domain, tools, and environment | Resume forwarding with little interpretation |
| Process discipline | Defined intake, calibration, feedback, and follow-up | Ad hoc communication and vague timelines |
| Market insight | Honest pushback on unrealistic requirements | Agreement with every requirement to win the business |
One option in this category is Nexus IT Group's healthcare IT recruiters and staffing specialists, which is structured around healthcare IT hiring rather than general recruiting. That matters only if the firm can demonstrate the role fluency and process discipline outlined above. The same standard should apply to every partner on the shortlist.
A good recruiting partner narrows ambiguity. A weak one amplifies it.
Signs the firm can handle a hard search
A short conversation often reveals whether the recruiter can manage a difficult market. Strong firms usually do three things early:
- They challenge the intake. If a CIO combines too many niche requirements into one role, the recruiter says so.
- They explain trade-offs. The firm identifies which qualifications are essential and which ones reduce the pool too sharply.
- They control the process. Candidate calibration, feedback loops, and hiring manager responsiveness get addressed before sourcing starts.
Healthcare IT recruiting firms earn their fee in the search design stage as much as in sourcing. If that stage feels thin, the rest of the engagement usually follows.
Selecting Your Recruitment Engagement Model
The same firm can be the right partner under the wrong commercial model. That's where many hiring teams lose time. They choose the cheapest structure on paper, then discover it doesn't fit the role's urgency, specificity, or decision path.
The practical choice usually comes down to contingency, retained, or contract-to-hire. None is universally better. Each works when it matches the hiring problem.
Choosing Your Engagement Model
| Model | Best For | Fee Structure | Key Advantage |
|---|---|---|---|
| Contingency | Mid-level roles with a broader candidate market and moderate urgency | Fee is typically due after a successful hire | Low upfront commitment |
| Retained | Executive, confidential, highly specialized, or business-critical searches | Payment is usually staged across the search | Deeper search commitment and tighter partnership |
| Contract-to-hire | Roles tied to uncertain headcount, project work, or skills validation before conversion | Candidate starts as a contractor, with conversion terms defined in advance | Lowers hiring risk before a permanent decision |
When contingency works
Contingency can fit roles that are still specialized but not board-level scarce. Think systems engineers, infrastructure leads, or healthcare application support roles where the search is difficult but not uniquely confidential.
This model works best when the organization can interview quickly and the recruiter can access a reasonably reachable market. It works poorly when the role definition is still moving or the hiring team needs heavy advisory support.
When retained is the better choice
Retained search fits leadership hires and narrow, business-critical searches. A CMIO, VP of Applications, EHR transformation leader, or cyber leader supporting hospital operations usually needs a more deliberate process. The candidate pool is often passive, the outreach needs discretion, and the assessment bar is higher.
In those cases, retained search buys commitment and focus. It also creates room for talent mapping, stakeholder alignment, and market feedback that a lighter model may not support.
If the organization would describe the role as “hard to replace if this goes wrong,” retained is often the safer model.
When contract-to-hire earns its keep
Contract-to-hire is often the most practical answer when the work is clear but the long-term seat is not. It's useful for implementation support, migration projects, interim leadership gaps, or teams testing whether a role should become permanent after a major initiative stabilizes.
For CIOs evaluating flexible options, recruitment as a service can also sit adjacent to these models when the need is ongoing hiring support rather than one isolated search. The key is to match the commercial structure to the operating reality, not to force every role into a standard direct-hire approach.
A simple selection lens
Use four filters before choosing:
- Urgency: Is the business absorbing active pain from the vacancy?
- Seniority: Does the role shape strategy or mostly execute within it?
- Specificity: How narrow is the required healthcare and technical overlap?
- Headcount certainty: Is this definitely a permanent seat, or still under evaluation?
The right engagement model should reduce friction, not create it.
Defining KPIs and SLAs for Your Recruiting Firm
A recruiting partnership becomes measurable when the hiring team stops tracking activity and starts tracking conversion. Resume count is activity. Qualified progression is performance.
That distinction matters even more in healthcare IT, where weak fits consume stakeholder time quickly. Healthcare recruiting guidance recommends tracking time-to-fill, cost-per-hire, and quality-of-hire, and notes that healthcare-sector turnover is roughly four times that of other industries, which makes retention a core KPI rather than a secondary HR metric.
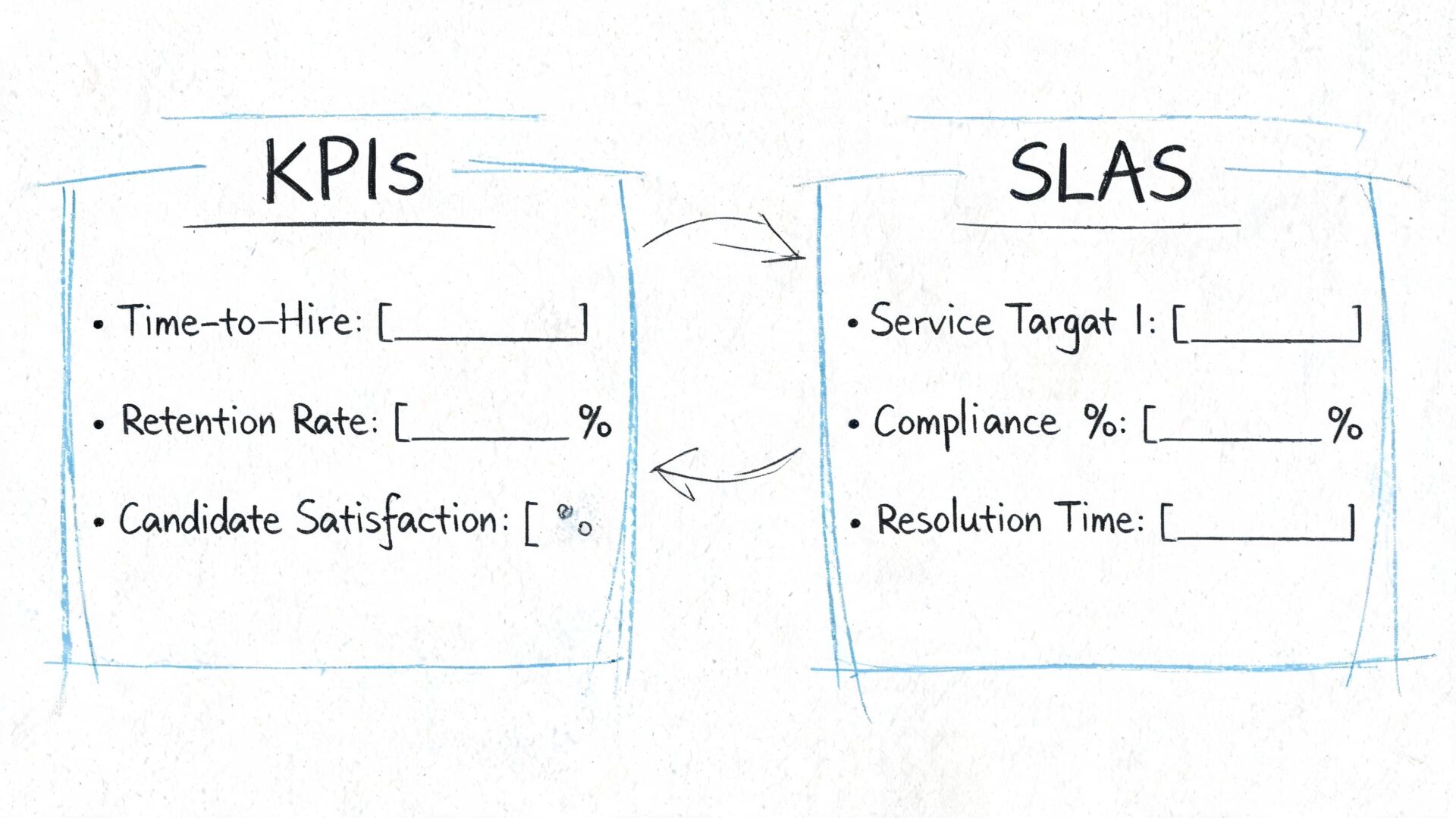
KPIs that show whether the search is working
The most useful KPI set is compact. It should show speed, quality, and staying power.
- Time-to-shortlist: How long it takes the firm to present the first qualified candidates.
- Submission-to-interview ratio: Whether the recruiter is calibrating quality correctly.
- Interview-to-offer ratio: Whether the hiring team and firm are aligned on the target profile.
- Time-to-fill: The overall measure of delivery against business urgency.
- Retention after placement: Whether the match held once the candidate entered the environment.
- Source effectiveness: Which channels are producing candidates that progress.
These metrics are more revealing than “resumes submitted” because they expose where friction lives. If shortlist speed is fine but interview conversion is poor, the problem may be role calibration. If offers are accepted but retention is weak, the issue may be candidate assessment or internal onboarding.
SLAs that prevent drift
SLAs should govern behavior on both sides. Many recruiting partnerships underperform because the agency has deadlines and the hiring team has none.
A practical SLA often covers:
| SLA area | Example expectation |
|---|---|
| Intake quality | Hiring team provides role scope, reporting line, must-haves, and interview process upfront |
| Candidate feedback | Interview feedback returned within an agreed window |
| Recruiter communication | Search updates delivered on a predictable cadence |
| Candidate handling | Recruiter confirms interest, compensation alignment, and availability before submission |
| Escalation path | Named contacts resolve delays, conflicts, or role changes quickly |
Operational note: If feedback loops are slow, even a strong recruiter will look ineffective because candidates lose confidence in the process.
What to avoid measuring
Some metrics create false confidence:
- Total resumes sent can reward noise.
- Raw outreach volume can reward spam.
- Job board traffic says little about whether the right people are engaged.
- Interview count alone can hide weak qualification.
The strongest healthcare IT recruiting firms welcome KPI discipline because it clarifies whether they're solving the actual hiring problem. If a firm resists measurable accountability, that's useful information before the relationship gets deeper.
Spotting Red Flags and Structuring the Agreement
Most failed recruiting engagements show warning signs early. The problem is that hiring teams often excuse them as normal search friction. In healthcare IT, that delay gets expensive fast because the role was already urgent enough to outsource.
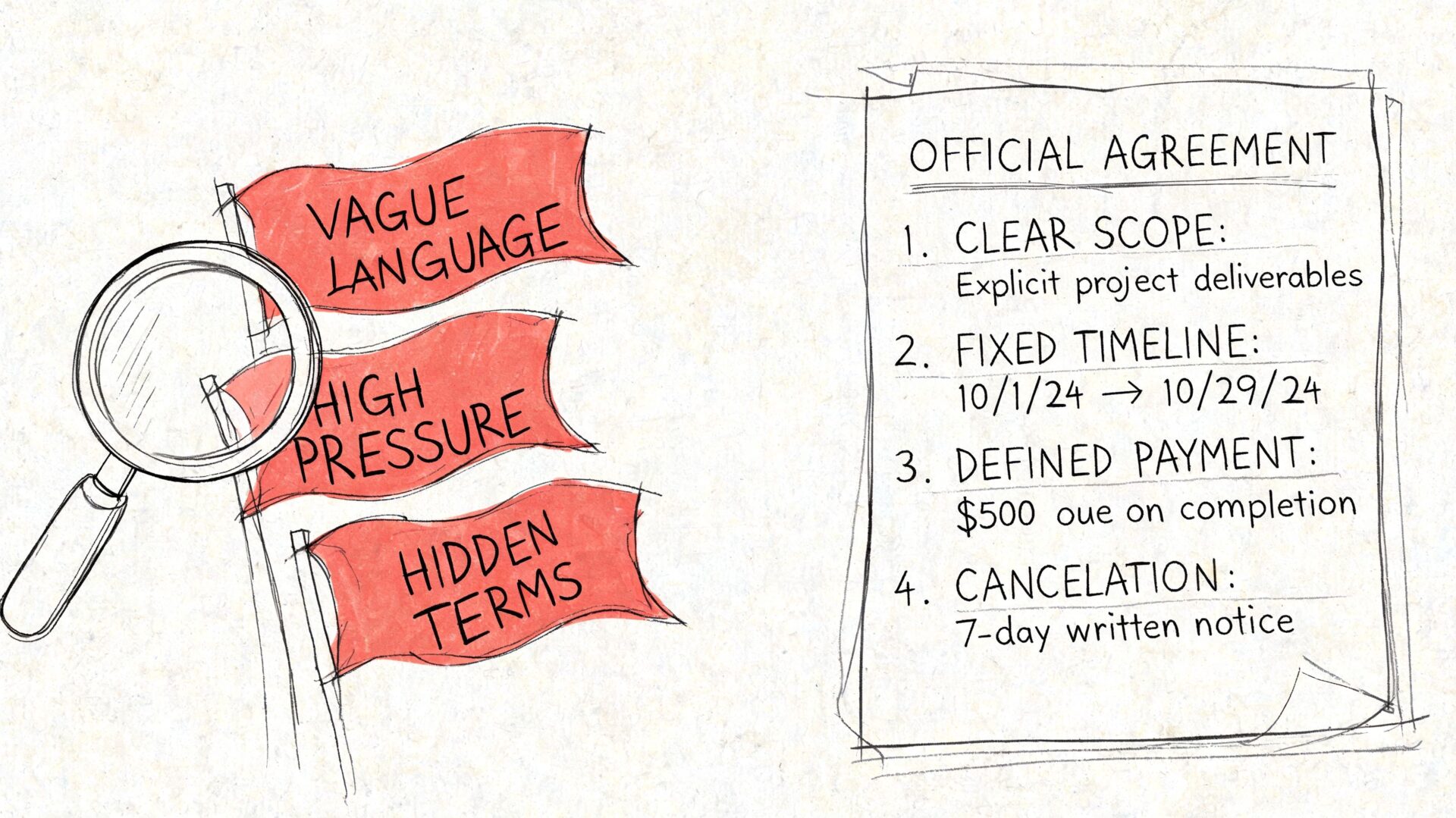
Red flags that usually get worse
A weak engagement often starts with one of these patterns:
- The recruiter avoids specificity. They talk about talent broadly but can't explain how they'll qualify healthcare domain fit.
- Candidate submissions feel interchangeable. Resumes arrive quickly, but the match logic is thin.
- The firm says yes to every requirement. Good partners push back when the combination of skills, setting, and compensation doesn't line up.
- Communication becomes reactive. Updates happen only when the client asks.
- The role keeps getting reinterpreted. If the recruiter still doesn't understand the environment after intake and calibration, candidate quality usually declines rather than improves.
A CIO shouldn't treat these signs as minor annoyances. They signal a search process that lacks structure.
Contract terms that matter in practice
The agreement should protect outcomes, not just payment mechanics. Several terms deserve close review.
- Guarantee period: If the hire leaves early, what happens next? The real question isn't whether a guarantee exists. It's whether the replacement or credit terms are clear and workable.
- Candidate ownership: The contract should define how long a submitted candidate remains tied to the firm. Ambiguity here causes disputes later.
- Fee trigger: Payment should be tied to a clear hiring event, with terms that reflect the chosen engagement model.
- Replacement process: If a search needs to restart, the path shouldn't require renegotiating every detail.
- Exclusivity language: Exclusive terms can help in the right search, but only when paired with real delivery expectations.
Weak contracts create friction at the worst moment, usually after a placement issue or a candidate ownership dispute.
The business lens for legal review
Legal teams naturally focus on wording. CIOs and talent leaders should focus on operational consequences. If the agreement doesn't support fast issue resolution, clear accountability, and a fair remedy when the search misses, it won't help much when pressure rises.
The cleanest contracts do two things well. They define the working rules before a problem appears, and they make it easy to decide what happens next.
From Vendor to Partner Your Long-Term Strategy
The strongest healthcare IT recruiting firms don't function as resume suppliers. They become part of the hiring system. They know which roles should go to external search, which ones internal talent acquisition can close, and where the organization keeps misjudging the market.
That's the decision framework. Start with vacancy cost, not fee sensitivity. Vet for domain fluency, not generic recruiting claims. Choose the engagement model that matches the role. Manage the partnership with KPIs and SLAs that measure quality and retention. Put the agreement on solid footing before urgency turns into avoidable conflict.
A CIO who handles recruiting this way gets more than placements. The organization gains better market feedback, a sharper view of role design, and a more realistic understanding of what healthcare IT talent will and won't accept. In a constrained market, that's a competitive advantage.
The right partner won't remove every hiring challenge. It will make the challenge legible, manageable, and less costly to solve.
If a team needs a recruiting partner that works specifically in technology hiring, nexus IT group is one option to evaluate alongside other healthcare IT recruiting firms. The right next step is a practical one. Bring one hard role, define the business impact of delay, and assess whether the firm can speak credibly about the work, the market, and the hiring process before any agreement is signed.